
A Case Report of Stroke in Secondary Hyperoxaluria
Article Sidebar
Main Article Content
Abstract
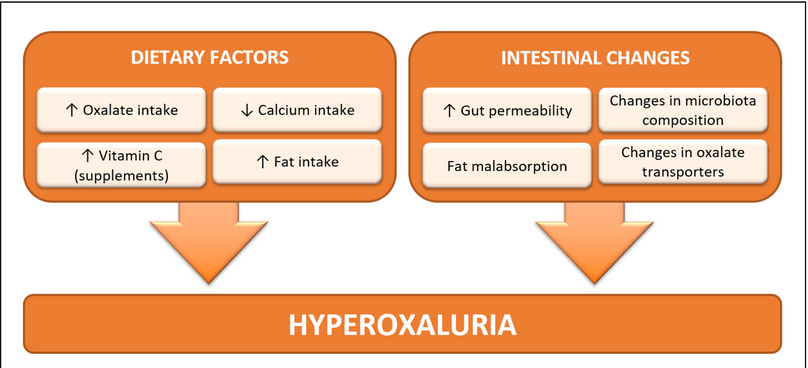
Hyperoxaluria is most common in developed countries like the USA, but not sporadic in developing countries. Hyperoxaluria is a state, that occurs when a patient has an excess of oxalate formation in urine. hyperoxaluria is of two types- Primary hyperoxaluria is due to an inherited defect of alanine glyoxalate transaminase. Secondary hyperoxaluria is due to increased GIT absorption of oxalates. In hyperoxaluria, there are increased oxalate levels in the blood, which get accumulate in joint spaces, tissues, and bone marrow resulting in systemic oxalosis. The conjunction of hyperoxaluria and CNS ischemia stroke is unusual
Here we are discussing a case of 71 years old male patient with a known case of Crohn’s disease for 20 years, with a history of small bowel resection 6 years back, with an intact colon, post-operatively not on regular medications. History of recurrent renal stones, history of insomnia, presented with CNS ischemic stroke
In this patient, there is an increased chance of secondary hyperoxaluria, due to raised absorbency of the large intestine to oxalates, which also increases blood oxalates levels, and there is a surge in accumulation of free oxalates in the large intestine lumen, due to fatty acids combined with luminal calcium. In patients with secondary hyper-oxalosis, that circulating oxalate precipitate could be a risk factor for stroke
Article Details
References
Worcester EM. Stones from bowel disease. Endocrinol Metab Clin North Am. 2002;31:979–999. [PubMed] [Google Scholar]
Holmes RP, Kennedy M. Estimation of the oxalate content of foods and daily oxalate intake. Kidney Int. 2000;57:1662–1667. [PubMed] [Google Scholar]
Holmes RP, Goodman HO, Assimos DG. Contribution of dietary oxalate to urinary oxalate excretion. Kidney Int. 2001;59:270–276. [PubMed] [Google Scholar]
Lemann J, Pleuss JA, Worcester EM, Hornick L, Schrab D, Hoffmann RG. Urinary oxalate excretion increases with body size and decreases with increasing dietary calcium intake among healthy adults. Kidney Int. 1996;49:200–208. [PubMed] [Google Scholar]
Hoppe B. An update on primary hyperoxaluria. Nat Rev Nephrol. 2012;8:467–475. [PubMed] [Google Scholar]
Rumsby G, Cochat P. Primary hyperoxaluria. N Engl J Med. 2013;369:2163. [PubMed] [Google Scholar]
Mittal RD, Kumar R. Gut-inhabiting bacterium Oxalobacter formigenes: role in calcium oxalate urolithiasis. J Endourol. 2004;18:418–424. [PubMed] [Google Scholar]
Hatch M, Cornelius J, Allison M, Sidhu H, Peck A, Freel RW. Oxalobacter sp. reduces urinary oxalate excretion by promoting enteric oxalate secretion. Kidney Int. 2006;69:691–698. [PubMed] [Google Scholar]
Dobbins JW Binder HJ . Importance of the colon in enteric hyperoxaluria. N Engl J Med1977; 296: 298–301
von Unruh GE Voss S Sauerbruch T et al. Dependence of oxalate absorption on the daily calcium intake. J Am Soc Nephrol2004; 15: 1567–1573
Robijn S Hoppe B Vervaet BA et al. Hyperoxaluria: a gut-kidney axis? Kidney Int 2011; 80: 1146–1158